








Model Guide | Mouse Myocardial Infarction (MI) Model Construction and Validation Methods
 source:ELK Biotechnology
source:ELK Biotechnology date:2026-06-15
date:2026-06-15 views:795
views:795
Background
Myocardial infarction (MI) is one of the major health threats worldwide and a leading cause of cardiovascular death and morbidity. Its pathogenesis involves partial or complete occlusion of coronary arteries, blocking blood flow to the myocardium, leading to local necrosis due to severe and persistent ischemia and hypoxia.
Mice, with their clear genetic background, short breeding cycle, and relatively mature surgical techniques, have become ideal experimental animal models for simulating human MI. By constructing this model, researchers can directly study key processes such as inflammatory response, fibrotic repair, and cardiac functional changes after myocardial ischemic necrosis under controlled conditions, providing a platform for drug screening, gene therapy, and regenerative medicine research.
Mouse MI Model Construction Method
The mainstream method is surgical ligation of the mouse coronary artery to simulate vascular occlusion. Below is a summary of key steps for the oral intubation thoracotomy ligation method:
▶ Experimental Materials:
• C57 mice (male, 6–8 weeks old)
• Avertin (manufacturer: Nanjing Aibei Biotechnology Co., Ltd.)
• General small animal anesthesia machine (manufacturer: RWD, model: R580S)
▶ Modeling Procedure:
1.Adaptive feeding for 7 days. Anesthetize mice with Avertin at 0.2 mL/10 g body weight.
2.Make a neck incision, bluntly dissect the trachea, perform oral intubation, and connect to a ventilator with preset parameters: respiratory rate 112 breaths/min, inspiratory/expiratory ratio 1:1, tidal volume 2.4 mL. Bluntly dissect the left chest muscles to expose the intercostal space. Tear open the muscles between the 3rd and 4th ribs to expose the heart. Gently tear a small opening in the pericardium. Use a 6-0 silk suture needle to ligate between the left atrial appendage and the aortic cone. ST-segment elevation on ECG indicates successful ligation. Then suture the intercostal muscles and chest muscles. Remove the ventilator after 5–10 minutes, wait for spontaneous breathing recovery, and place the mouse back in its cage.
3.Collect samples 1–2 weeks after modeling.
▶ Evaluation Indicators: TTC staining, Masson staining, HE staining, ELISA
1. Model Validation
♦ TTC Staining
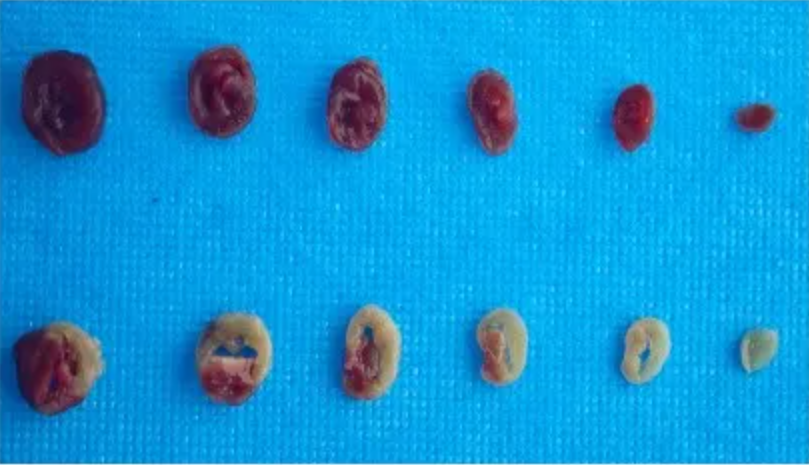
TTC staining result: Dehydrogenase in viable cardiomyocytes reduces TTC to a red color, while necrotic myocardium appears pale due to loss of enzyme activity.
♦ Masson Staining
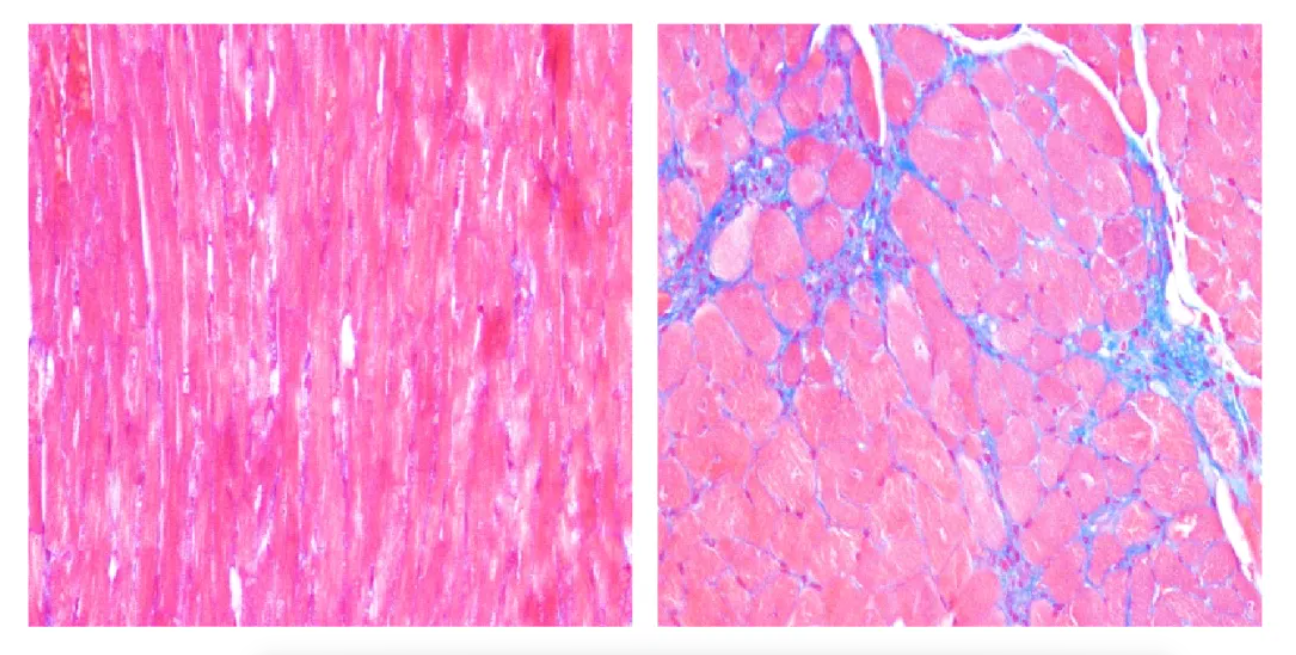
Masson staining result: Collagen fibers are stained blue, cardiomyocytes red. In the normal group, a small amount of collagen is present in the intercellular space and around blood vessels. In the model group, tissue structure is abnormal, with myocardial and interstitial fibrosis, blue collagen deposition, and local fibrous scar formation between myocardial tissues. This is a key method for evaluating myocardial fibrosis.
♦ HE Staining
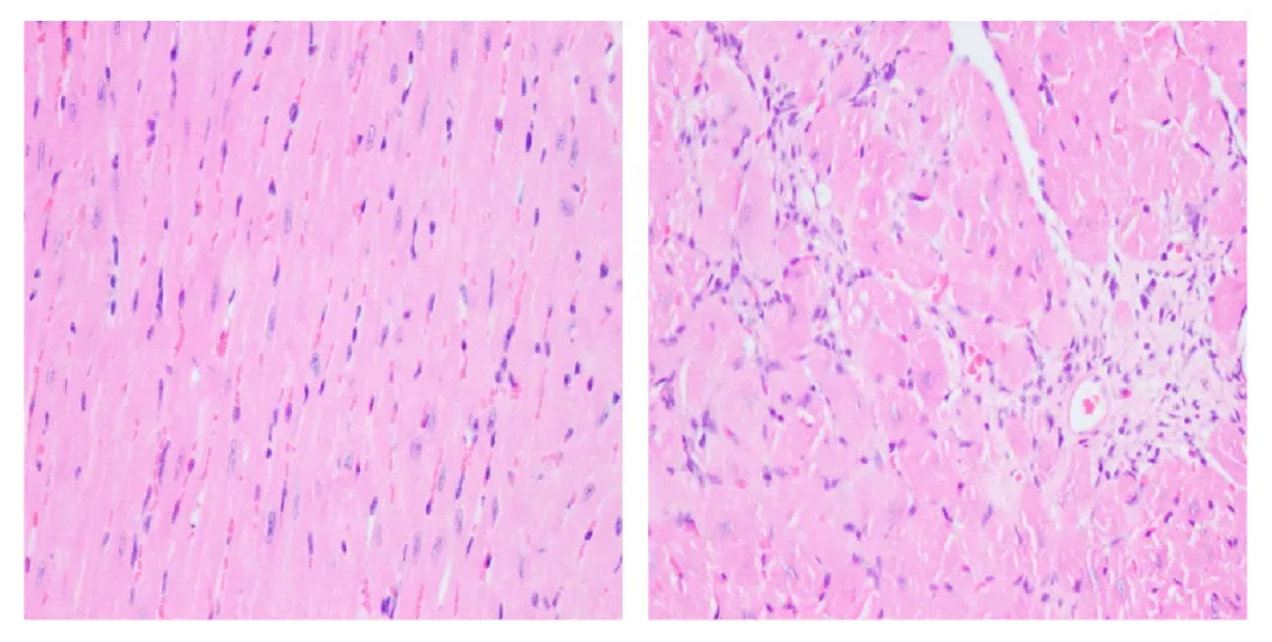
HE staining result: Compared with the normal group, the model group shows loose and edematous tissue, inflammatory cell infiltration, capillary proliferation; necrotic muscle fibers are replaced by loose fibrous connective tissue, and some fields show obvious vasodilation.
♦ ELISA Detection
ELISA results: Serum MYO and CK-MB concentrations in the model group were significantly higher than those in the normal group, validating the effectiveness of this modeling method.
Common ELISA Detection Indicators for Acute Myocardial Infarction (AMI)
In model construction and related mechanism studies, ELISA detection of specific protein levels in serum or tissues is an important means to quantitatively assess myocardial injury, inflammatory status, and prognosis. ELK Biotechnology provides a list of commonly used ELISA detection indicators, categorized by early markers, definitive markers, inflammation/oxidative stress, cardiac function/fibrosis, and prognosis/plaque-related markers. All are commonly measurable by ELISA in preclinical animal cell and serum samples.
Core Gold-Standard Diagnostic Markers for MI (Most Commonly Used)
1.cTnI – Cardiac troponin I
Highest specificity, MI-specific marker, rises early and persists for a long time. Classic ELISA indicator.
2.cTnT – Cardiac troponin T
Similar to cTnI, myocardial-specific injury marker, assesses extent of myocardial necrosis.
3.CK-MB – Creatine kinase isoenzyme MB
Traditional MI marker, reflects myocardial cell damage, quantifiable by ELISA.
4.Myoglobin – The earliest rising MI marker, increases within 1–2 hours of onset, suitable for early screening.
Inflammation & Immune-Related ELISA Indicators (MI Inflammatory Response)
TNF-α, IL-1β, IL-6, IL-8, IL-10
ELISA Validation for MI Model Construction:
Must include: cTnI + CK-MB + Myoglobin

 RETURN
RETURN