








Inflammatory Factor TNF-α: How It Shapes Immunity, Tumors and Autoimmune Diseases
 source:ELK Biotechnology
source:ELK Biotechnology date:2026-07-03
date:2026-07-03 views:296
views:296
I. From an Accidental Discovery to a Star Molecule
In the 1970s, while investigating tumor immunity, scientists observed that certain bacterial infections could trigger hemorrhagic necrosis in mouse tumors. In 1975, researchers led by Carswell at the Memorial Sloan Kettering Cancer Center (MSKCC) isolated a tumor-necrotizing factor from serum of mice treated with Bacillus Calmette-Guérin (BCG) and lipopolysaccharide (LPS), and named it Tumor Necrosis Factor (TNF).
Subsequently, the full-length cDNA of mouse and human TNF was cloned in 1984, and recombinant TNF protein was obtained, marking the official entry of this molecule into the field of molecular immunology. In 1985, TNF-α and TNF-β (LT-α) were formally distinguished.
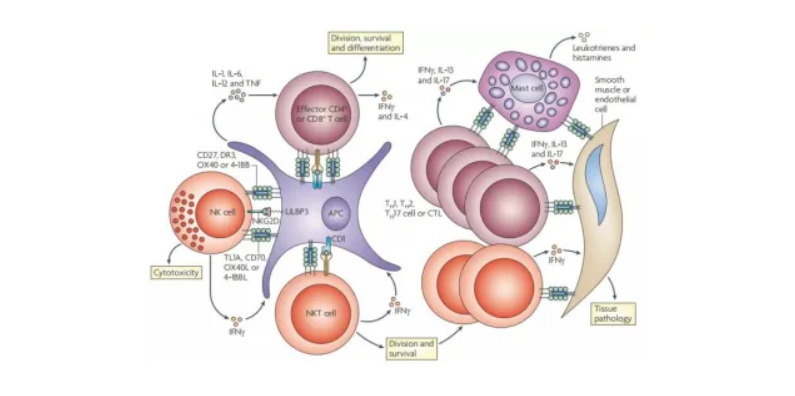
Primarily secreted by activated macrophages, monocytes and T cells, TNF-α serves as the prototype member of the TNF Superfamily (TNFSF). To date, this superfamily encompasses 19 ligands and 29 receptors, participating in the regulation of cell proliferation, differentiation, apoptosis and inflammation. The discovery of TNF-α not only uncovered the complex crosstalk between the immune system and tumors, but also laid the groundwork for the subsequent development of anti-TNF therapies.
II. TNF-α Signaling: Two Pathways, Two Distinct Cellular Fates
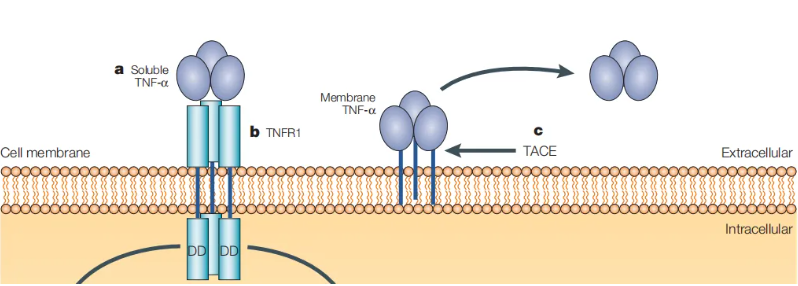
TNF-α exists as a homotrimer and binds predominantly to two receptors: TNFR1 (p55) and TNFR2 (p75). Despite sharing the same ligand, the two receptors mediate vastly different biological effects.
-
TNFR1: Expressed ubiquitously across nearly all cell types, it acts as the primary transducer of TNF-α-induced pro-inflammatory and pro-apoptotic signals. Upon ligand binding, the intracellular death domain (DD) of TNFR1 recruits adaptor molecules including TRADD, RIPK1 and TRAF2 to form Complex I, which activates the NF-κB and MAPK pathways to drive the expression of inflammatory genes. Under altered cellular conditions, Complex I can convert into Complex II, which activates caspase-8 to initiate apoptosis. When caspase activity is suppressed, RIPK1/RIPK3/MLKL-dependent necroptosis becomes an alternative cell death modality.
-
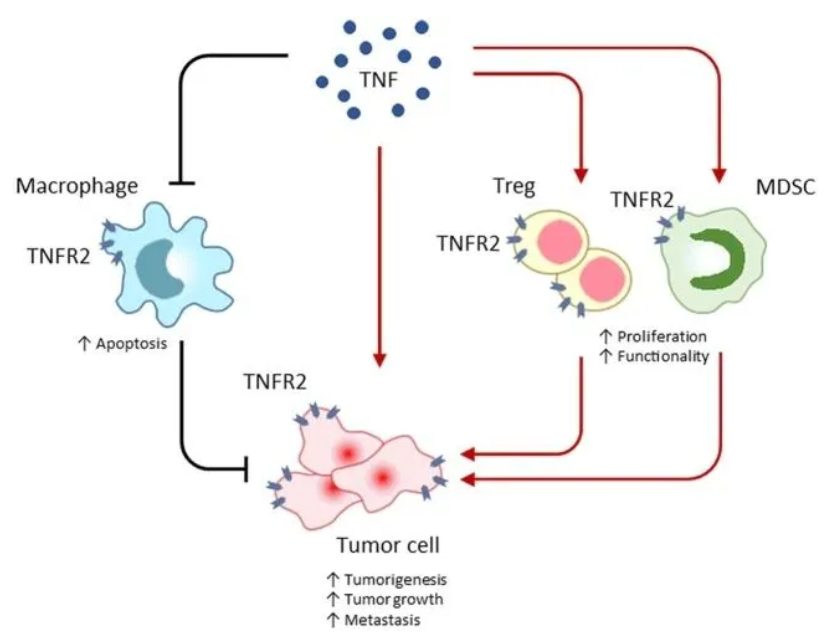
TNFR2: Mainly expressed on immune cells, endothelial cells and certain neurons. It recruits TRAF2/cIAPs to activate NF-κB, promoting cell survival, proliferation and tissue repair. Highly expressed on regulatory T cells (Tregs) and myeloid-derived suppressor cells (MDSCs), TNFR2 contributes to the establishment of immune-suppressive microenvironments.
This signaling architecture featuring "one ligand, two receptors and multiple biological outcomes" renders TNF-α an exquisite double-edged sword in immune regulation.
III. Physiological Functions of TNF-α: Immune Sentinel and Tissue Repair Mediator
Under physiological conditions, TNF-α acts as the first line of defense against infections and tissue injuries, exerting protective effects through the following mechanisms:
-
Activating immune cells: Stimulates the activation and chemotaxis of macrophages, neutrophils and dendritic cells, enhancing their phagocytic capacity and antigen presentation.
-
Inducing acute-phase response: Stimulates hepatocytes to synthesize C-reactive protein (CRP) and serum amyloid A (SAA), orchestrating systemic inflammatory responses.
-
Regulating tissue repair: After skin, intestinal and hepatic injury, TNF-α facilitates fibroblast proliferation, angiogenesis and matrix remodeling to accelerate wound healing.
-
Maintaining immune homeostasis: Modulates Treg differentiation and effector T cell responses to prevent excessive immune-mediated tissue damage.
Nevertheless, dysregulated production or aberrant signaling of TNF-α transforms it from a protective sentinel into a destructive mediator.
IV. The Dual Role of TNF-α in Diseases
1. Autoimmune Diseases: From Protector to Autologous Attacker
TNF-α is a core driver of rheumatoid arthritis (RA), inflammatory bowel disease (IBD), psoriasis, ankylosing spondylitis and other autoimmune disorders. In the synovial tissue of RA patients, overexpressed TNF-α triggers abnormal proliferation of fibroblast-like synoviocytes, osteoclast activation and cartilage erosion. Clinical data demonstrate that anti-TNF biologics (e.g., infliximab, adalimumab) significantly alleviate symptoms and retard joint destruction, establishing them as first-line therapies for RA and IBD.
2. Tumors: Tumor-Suppressive or Oncogenic?
The function of TNF-α in tumors is highly context-dependent on the tumor microenvironment. High concentrations of TNF-α can directly induce apoptosis or necrosis in tumor cells, the very property that inspired its original nomenclature. In contrast, chronic low-level TNF-α activates NF-κB to promote tumor cell survival, epithelial-mesenchymal transition (EMT) and angiogenesis, while recruiting MDSCs and tumor-associated macrophages (TAMs) to suppress anti-tumor immunity. Multiple studies have linked elevated TNF-α expression to poor prognosis in breast, colorectal and liver cancers.
3. Infection and Sepsis
During severe infection or sepsis, massive TNF-α release triggers a cytokine storm, resulting in vascular leakage, multiple organ failure and even death. Early clinical trials investigating anti-TNF antibodies for sepsis yielded limited therapeutic efficacy, indicating that TNF-α’s role in infectious pathologies is far more complex than initially hypothesized.
4. Metabolic Disorders
TNF-α is a key mediator of obesity-induced insulin resistance. TNF-α secreted by adipose tissue macrophages disrupts insulin signaling and inhibits GLUT4 translocation, reducing peripheral tissue insulin sensitivity. While anti-TNF treatment improves glycemic control in type 2 diabetes animal models, human clinical trials have produced inconsistent outcomes.
V. Targeting TNF-α: From Monoclonal Antibodies to Small-Molecule Inhibitors
Since the FDA approved infliximab for Crohn’s disease in 1998, five generations of anti-TNF biologics have been developed:
-
Infliximab: Chimeric monoclonal antibody, intravenous administration
-
Adalimumab: Fully human monoclonal antibody, subcutaneous injection
-
Etanercept: TNFR2-Fc fusion protein, soluble receptor decoy
-
Golimumab: Fully human monoclonal antibody, subcutaneous injection
-
Certolizumab pegol: PEGylated Fab fragment, subcutaneous injection
Widely prescribed for RA, IBD, psoriasis, ankylosing spondylitis and uveitis, these agents generate annual global sales exceeding 40 billion US dollars. However, long-term administration carries risks including increased susceptibility to infections, immunogenicity and non-response in a subset of patients.
In recent years, small-molecule TNF-α inhibitors have emerged as a prominent research focus. For instance, SPD304 disrupts TNF-α homotrimer assembly, while XPro1595 selectively neutralizes soluble TNF-α. Additionally, inhibitors targeting downstream signaling molecules such as TACE (ADAM17), RIPK1 and MAPK are under preclinical or early-phase clinical evaluation.
VI. Future Outlook: Precision Modulation of TNF-α
The dual-sided activity of TNF-α suggests that non-selective full blockade may not represent the optimal therapeutic strategy. Key research directions for the future include:
-
Selective targeting of TNFR1 versus TNFR2: Block pro-inflammatory TNFR1 signaling while preserving TNFR2-mediated immune regulatory functions.
-
Local delivery systems: Nanocarriers or antibody-drug conjugates (ADCs) to achieve targeted delivery of TNF-α inhibitors and minimize systemic side effects.
-
Combination therapy: Co-administration of anti-TNF agents with IL-17, IL-23 or JAK inhibitors to cover broader inflammatory signaling cascades.
-
Biomarker-guided personalized treatment: Predict patient therapeutic responses via genetic polymorphisms, serum TNF-α levels or receptor expression profiles to realize precision medicine.
VII. Conclusion
From its initial discovery in 1975 to its current status as a core therapeutic target in immunology, the research journey of TNF-α epitomizes translational progress spanning basic immunology and clinical medicine. It functions as a potent defensive sword against pathogens, yet may turn into an endogenous harmful toxin when its activity spirals out of control. Deciphering the sophisticated regulatory network of TNF-α signaling and developing more precise, safer intervention strategies poses both challenges and opportunities for today’s research scientists.
About Kelu Biotechnology
ELK Biotechnology has long focused on research into the TNF-α signaling pathway. We provide functionally validated recombinant TNF-α proteins, TNFR1/TNFR2 products, antibodies targeting TACE and downstream signaling molecules, as well as ELISA detection kits to support research on inflammatory mechanisms, tumor immunity and drug screening.

 RETURN
RETURN